Vorgeschichte
Wie schon im letzten Jahr, so hat Novapura auch dieses Jahr wieder eine Umfrage in Schweizerischen Gesundheitseinrichtungen durchgeführt. Titel der diesjährigen Umfrage: Wie werden Flächendesinfektionen im Schweizerischen Gesundheitswesen durchgeführt?
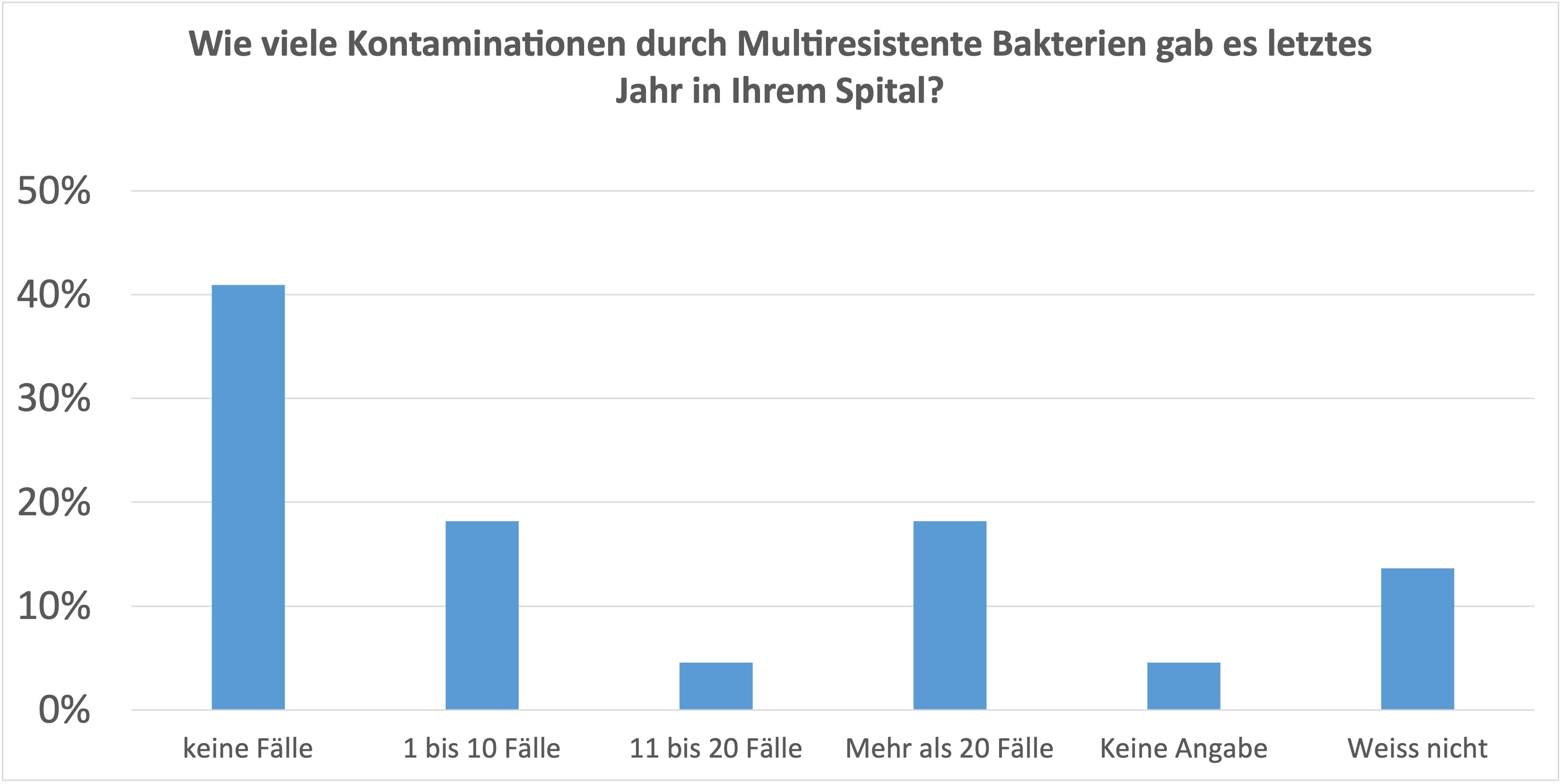
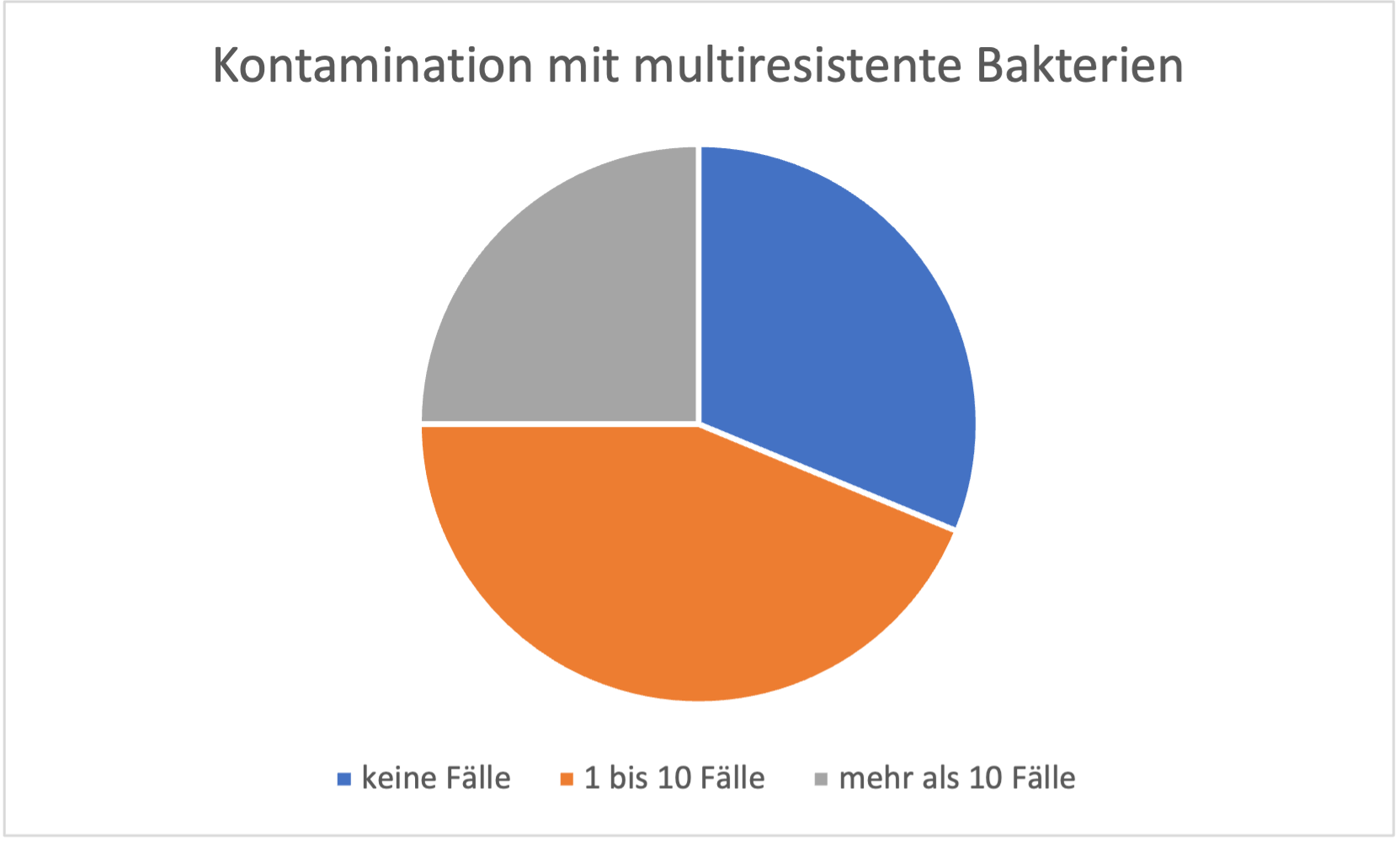
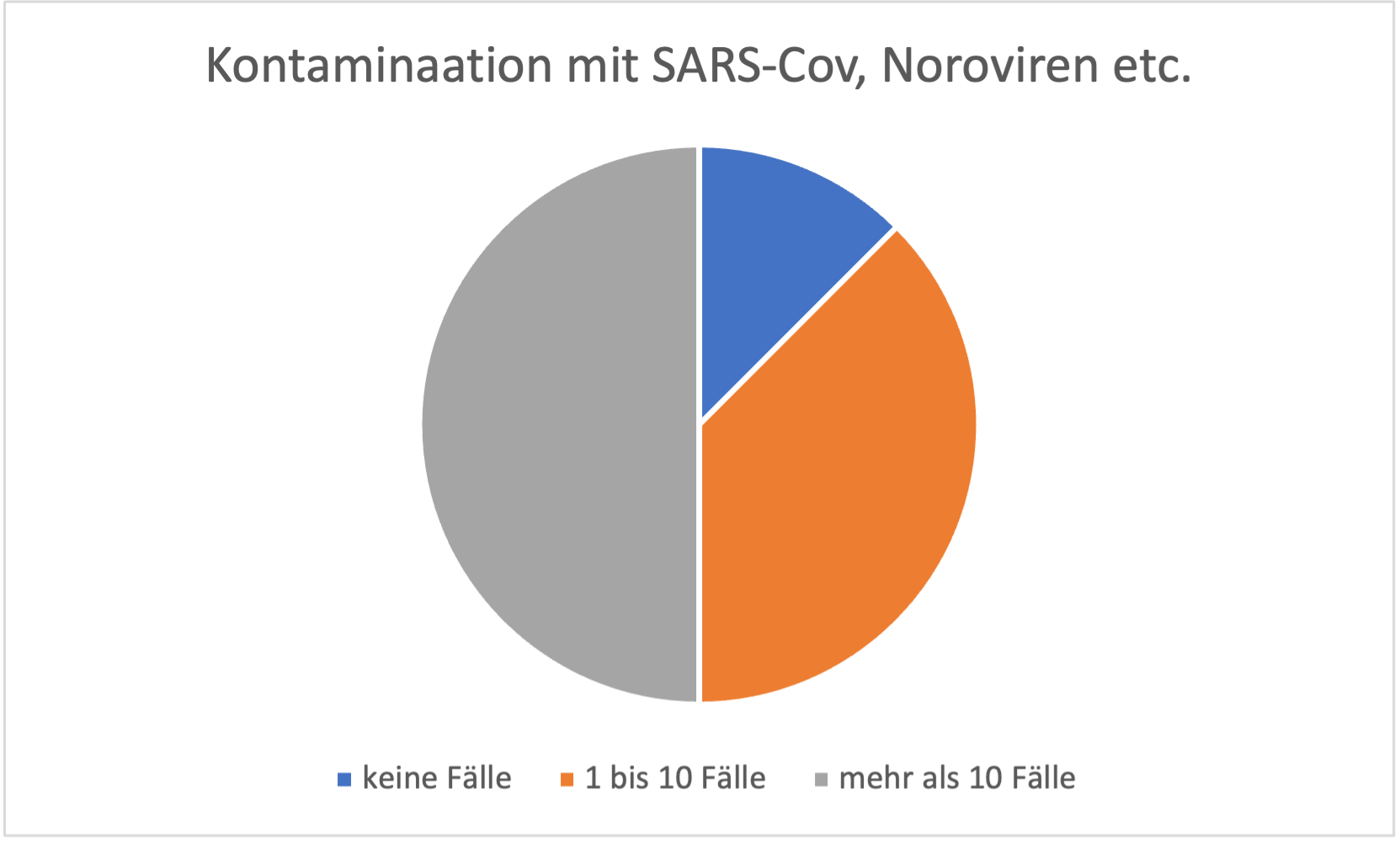
Die Anzahl Kontaminationen ist nach wie vor in fast allen Institutionen signifikant, insbesondere, wenn man die Fälle von multiresistenten Bakterien isoliert betrachtet.
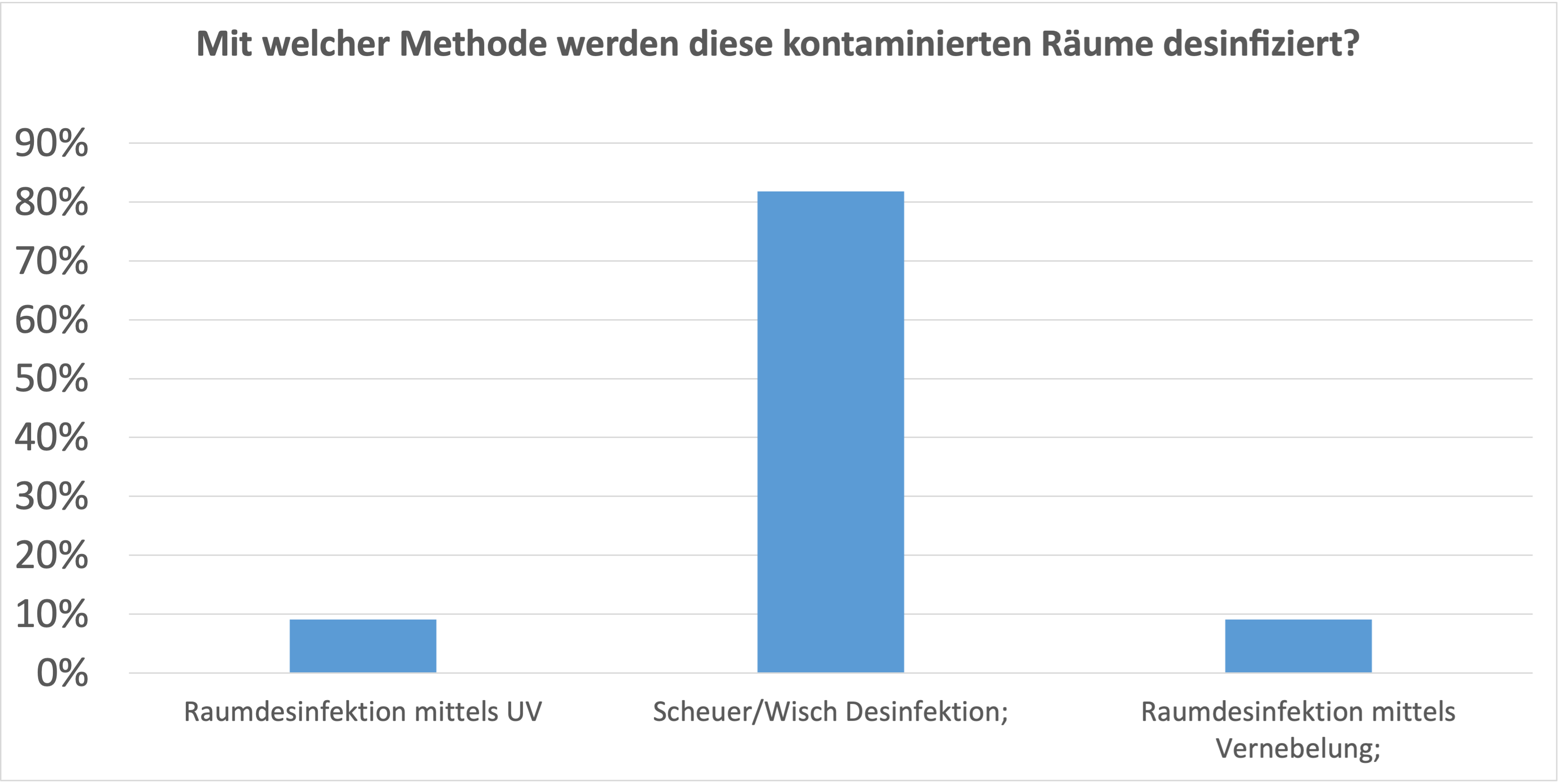
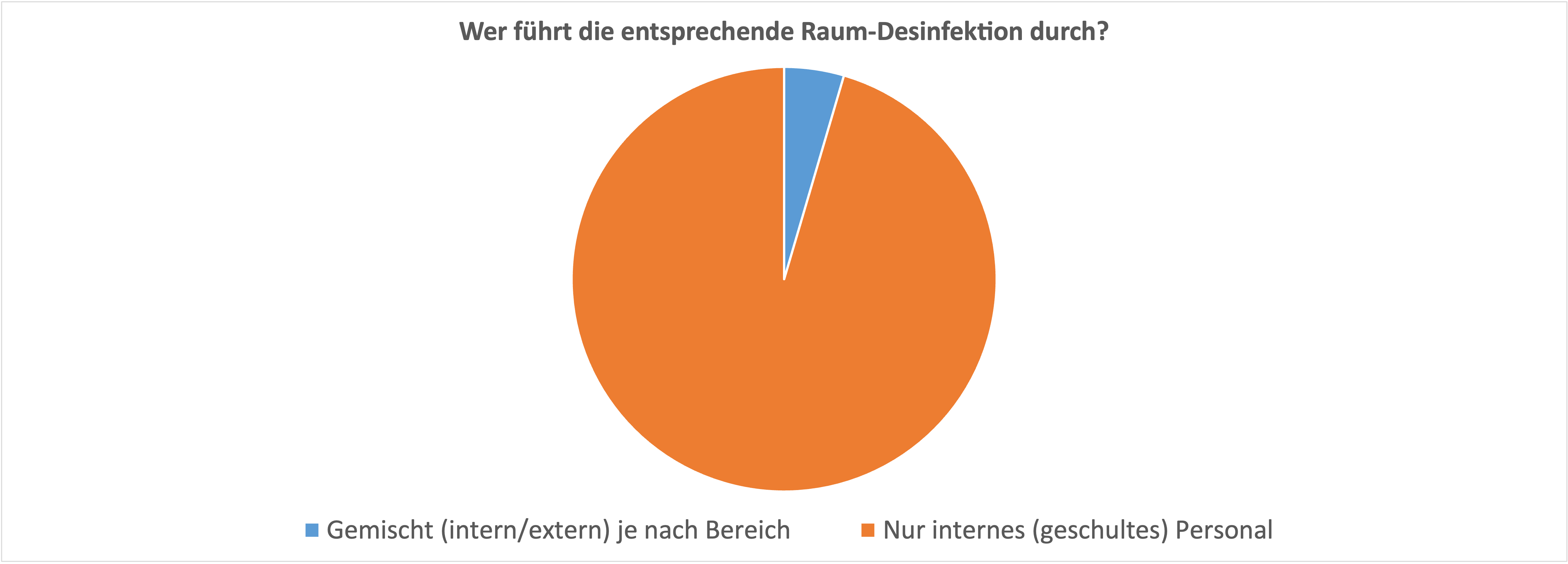
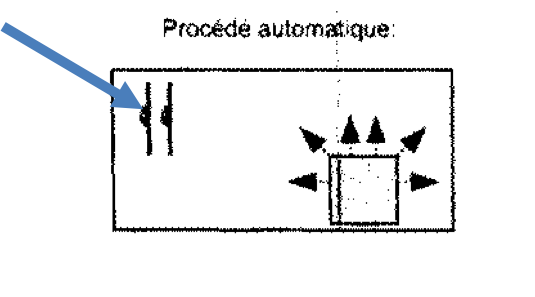
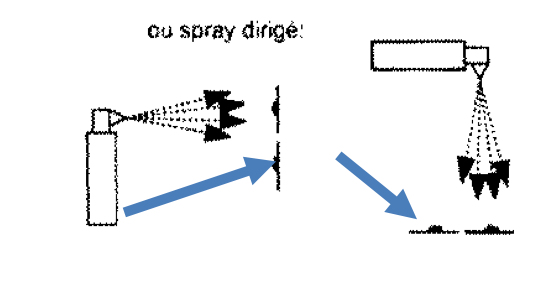
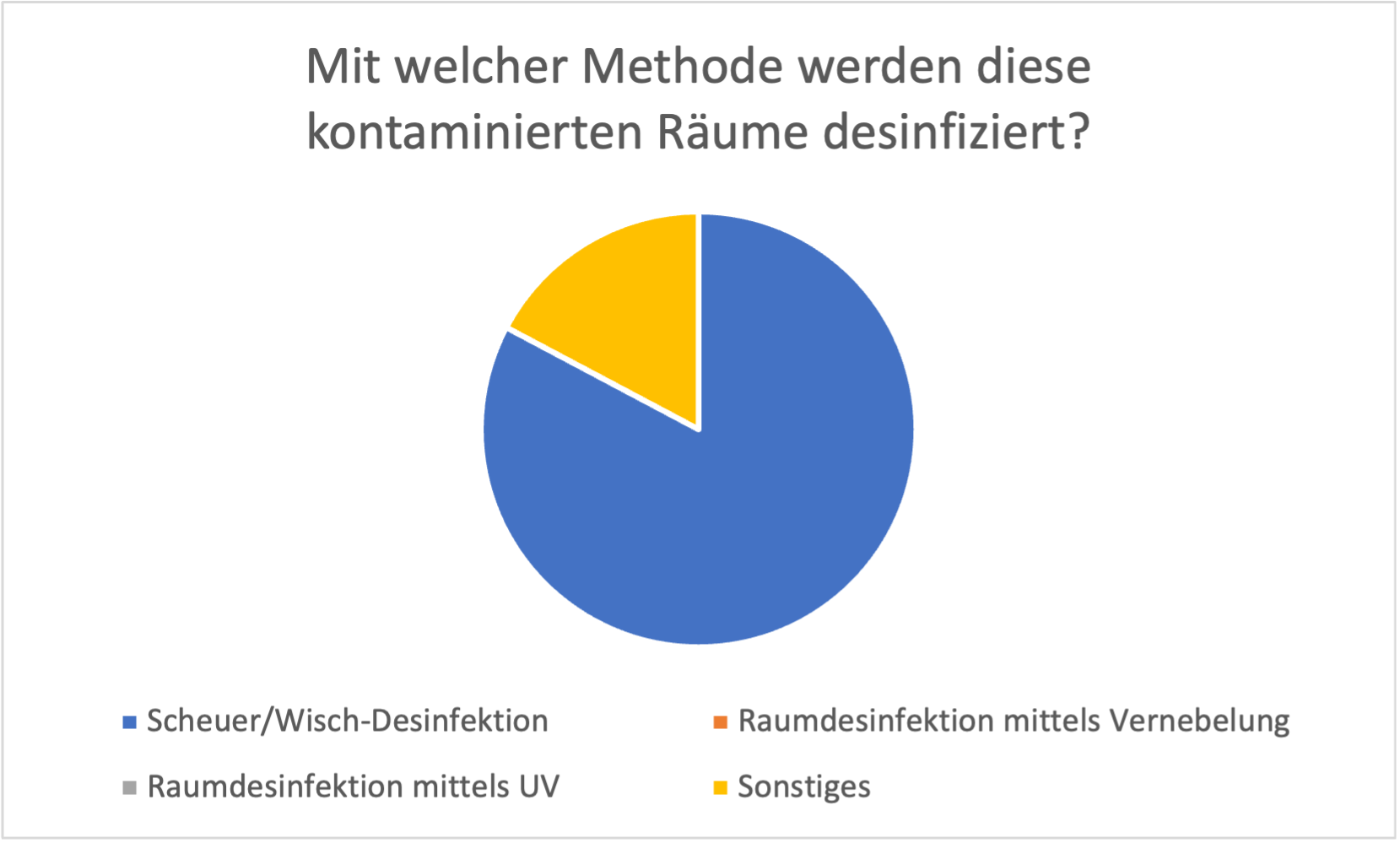
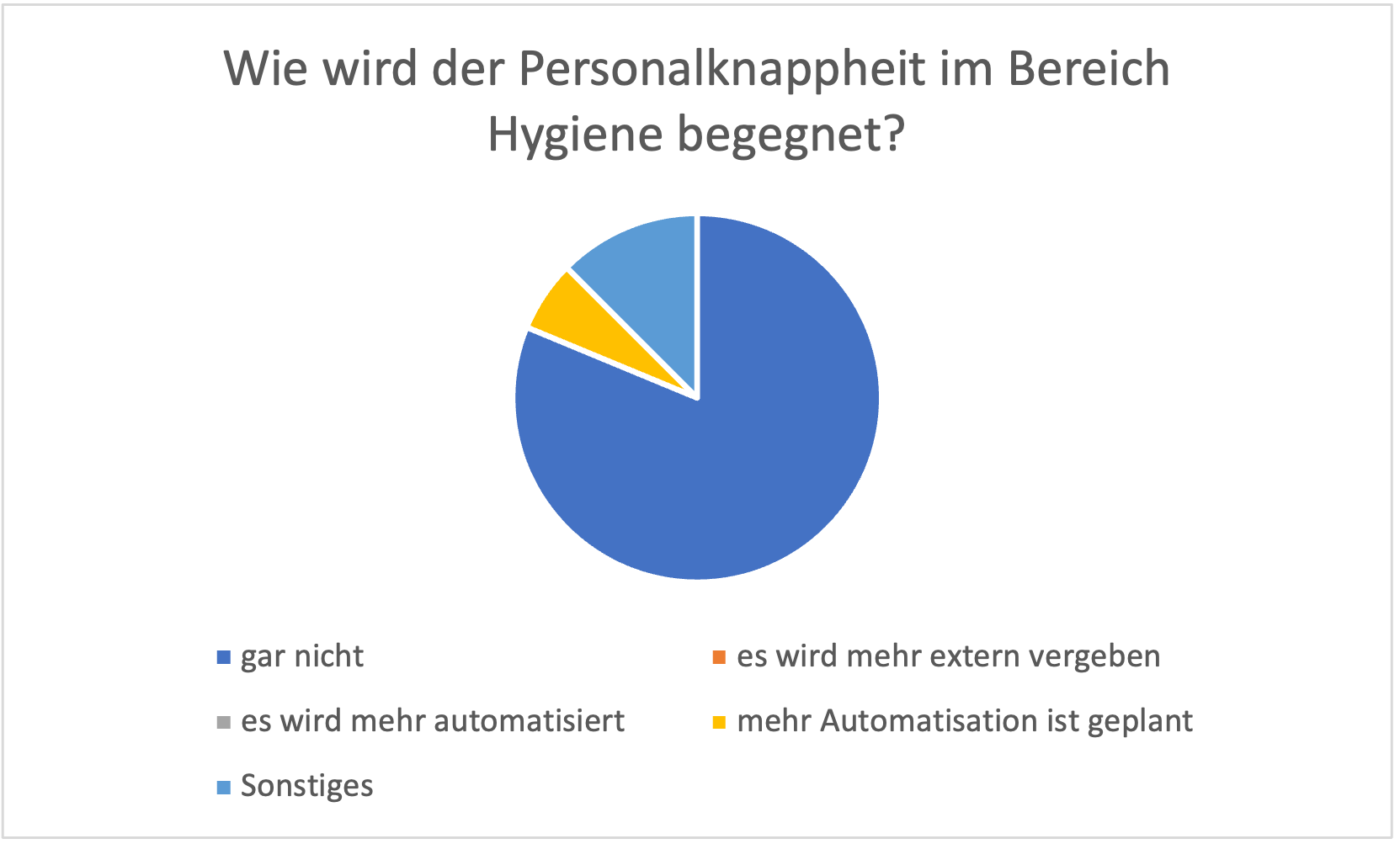
Kontaminiert wurden im wesentlichen Patientenzimmer und Quarantänezimmer, in einem geringeren Ausmass die Notfallaufnahme. Die Scheuer-/Wischdesinfektion ist nach wie vor die Methode der ersten Wahl, wenn es um die Dekontamination dieser Räume geht. In wenigen Fällen werden andere Methoden verwendet, wie z.B. Vernebelung. Zur Hauptsache wird internes, geschultes Personal auf diese Arbeiten angesetzt, trotz Personalmangel. Letzterem wird offenbar von Seiten der Institutsleitung nicht grosse Beachtung geschenkt. Laut den eingegangenen Antworten wird aber auch nicht auf eine Effizienzsteigerung durch Automatisation oder Outsourcing hin gearbeitet.
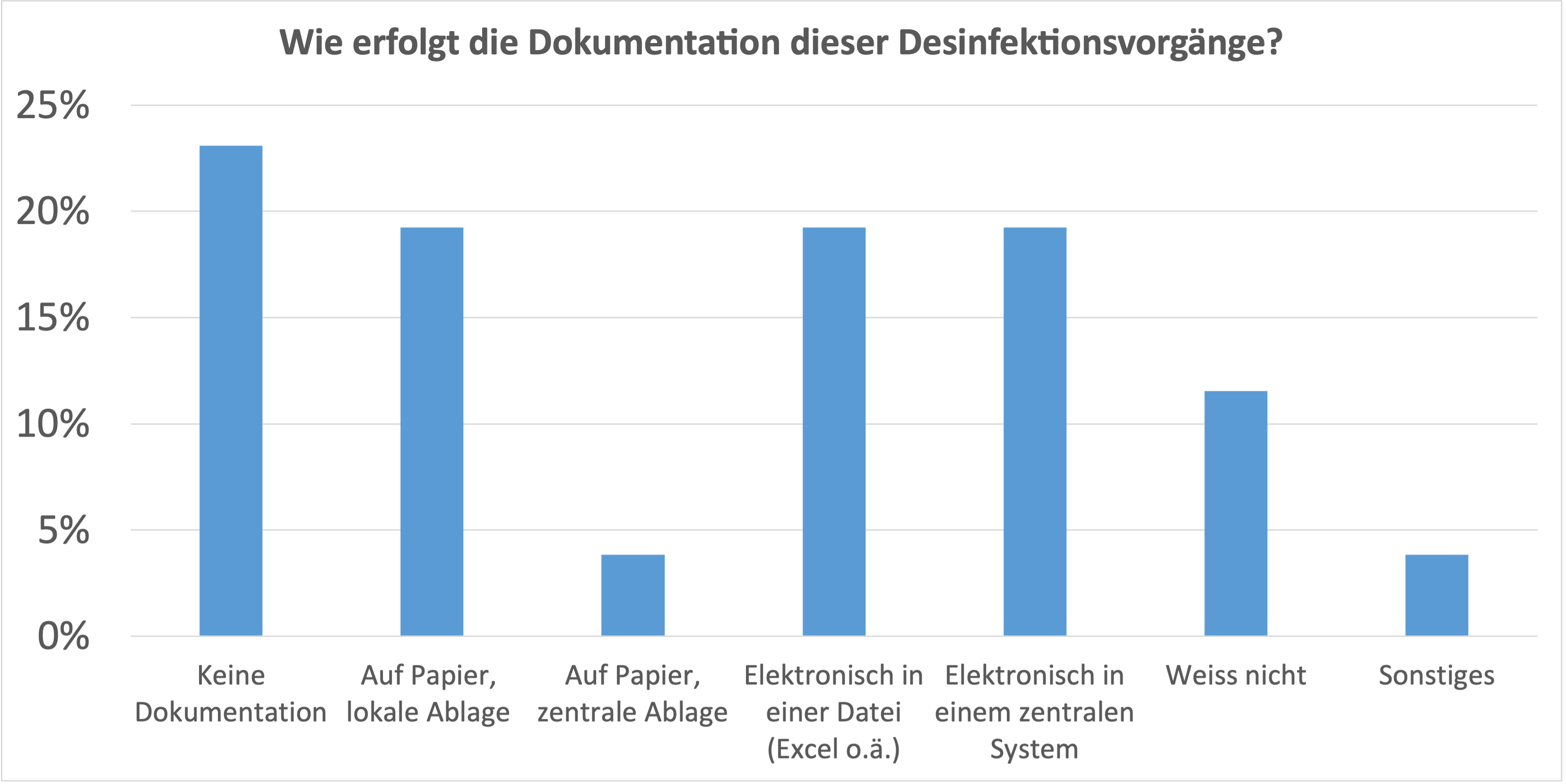
Dokumentiert und kontrolliert werden Dekontaminationen bei nur knapp 25% der Institutionen.
Welche Bereiche sind Ihrer Meinung nach kritisch bezüglich Kreuzkontamination? Zu dieser Frage werden im Wesentlichen Patientenzimmer und Notfallaufnahme genannt. Die Stationsküche, sowie die Bekleidung des Personals findet auch Erwähnung. Diese Angaben sind mit grosser Wahrscheinlichkeit nicht mit Messresultaten unterlegt.
Besonderes Augenmerk wird bei der Flächendesinfektion auf High Touch Flächen gelegt (Türgriffe, Handläufe, Griffe, Taster, Knöpfe etc.). Die Raumluft (wahrscheinlich aus der Zeit der Pandemie) findet auch Aufnahme in die Statistik. Bei High Touch Flächen ist die Scheuer-/Wischdesinfektion die Methode der ersten Wahl. Diese Flächen werden bis zu 3 Mal pro Tag desinfiziert; es gibt Institutionen, welche weniger als einmal pro Tag desinfizieren.
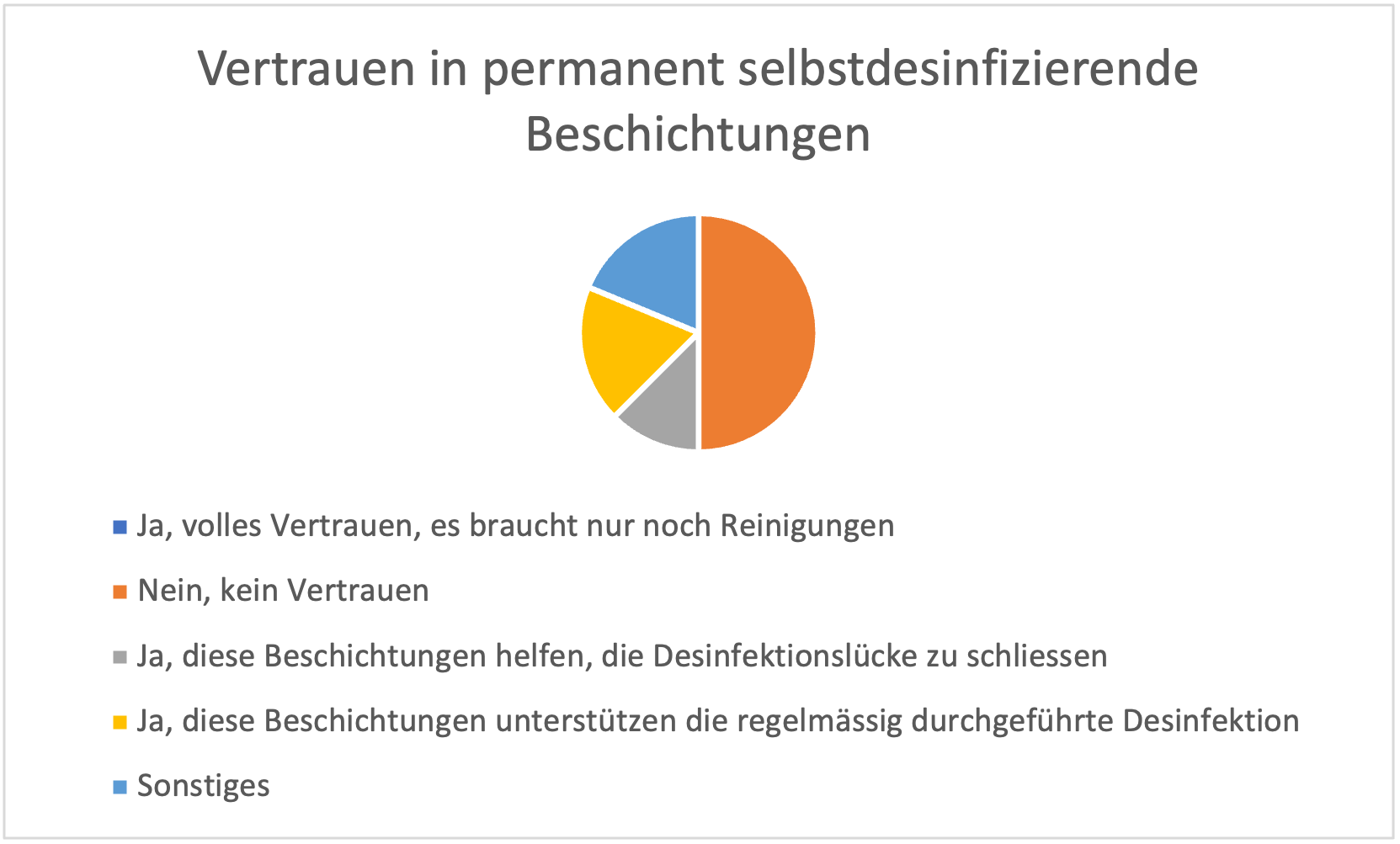
Hätten Sie Vertrauen in Beschichtungen mit permanent selbstdesinfizierenden Eigenschaften für High Touch Areas? 50% der Antworten fallen negativ aus, die anderen 1/3 sehen einen Benefit (Schliessen der Desinfektionslücke, Unterstützung bei der regelmässigen Desinfektion).
Mit welchen zusätzlichen, einfachen Massnahmen könnte man die Kreuzkontamination weiter eindämmen? Hier wird die gute alte Händedesinfektion zur Hauptsache genannt.
Zusammenfassung:
Methoden: Nach wie vor, analog der Umfrage des letzten Jahres, ist die Scheuer-/Wischdesinfektion die am häufigsten verwendete Methode zur Flächendesinfektion. Kontaminationen mit multiresistenen Bakterien, resp. SARS-Cov/Noro kommen gehäuft vor. Neue Technologien, wie Vernebelungsverfahren, UV-Roboter, selbstdesinfizierende Beschichtungen sind wenig verbreitet, resp. werden mit einer gewissen Skepsis begegnet oder sind gänzlich unbekannt. Der Personalmangel wird als grosses Problem angeschaut, welches offenbar nicht oder zu wenig energisch angegangen wird.